Biomedical science moves from one hot fashion to the next. A new technology emerges, investigators jump on the bandwagon and pitch it to the general public as the next great thing: a way to cure this, that or the other disease. I don't think the public understands just how extremely difficult it is to advance even the best ideas to a point where they have any hope of being transformed into a therapy, let alone the enormous difficulty of developing a therapeutic agent. We work with immensely complex systems (cells, tissues, the entire body) and, frequently, do not even have a halfway decent blueprint of the systems we're trying to manipulate.
Back when I started, the flavor of the month was gene therapy. Later, antisense, siRNA and genomics all had their moment in the spotlight. The beautiful thing is that these approaches sometimes pay off: it just takes a lot of time and slow, painful, grinding research. Often, they don't. Monoclonal antibodies were the hot new thing for drug development in the early 1980s, making the covers of Newsweek and Fortune in 1985. They faded from the public limelight, but investigators and biotech companies kept plugging away and, in 1997, important new therapies for cancer and autoimmune diseases based on humanized monoclonal antibodies began to emerge. It has been exciting and gratifying to watch the steady roll-out of important antibody-based therapies. Gene therapy, on the other hand: well, that's been a different story.
Which brings me to to stem cells. In 2001, the Bush administration severely limited research using human-embryo-derived stem cells. In response, in 2004, a group of activists sold California voters on the promise of the sexy new technology of "regenerative" medicine. California voters--perhaps a bit too trusting--jumped on the bandwagon, passing proposition 71 to fund the research. Scientists were heavily involved in making the pitch, most notably scientists who would directly benefit from this source of new grant funds (though they didn't make any great efforts--not any effort at all really--to point this out). Oh, by the way, how many lines of text in print advertisements or in scripts for TV and radio commercials did the proponents devote to conveying how challenging it would be to actually develop therapies? Or informing the lay public that stem cell-based therapies might not pan out at all? Here's one hint: a central topic of one of the first stem-cell planning meetings held at my institution after Prop 71 passed was how to dampen down the very expectations that the campaign had raised way, way too high.
In 2009, restrictions on federal funding of human embryonic stem cell funding were dropped. Also, new sources of stem cells not involving human embryos have been developed. The California agency doling out the stem cell research funds (CIRM, California Institute for Regenerative Medicine), has finite access to borrowed money and will award its last grants in 2017.
The good news is that the federal restrictions are gone: now stem cell researchers can compete on equal footing with researchers taking other approaches to finding cures. Since their approach is so promising, they should feel confident that their proposals will fare well in the grant application review scrum. Oh, wait, surprise! They are already making noises about wanting the good people of California--already some of the most highly taxed in the nation--to sell more bonds to support more research. Whose research? Theirs of course! Why compete for funding with investigators trying to cure cancer, nerve injury, diabetes etc with different approaches when you can pitch your story right to the well-meaning voters, going through an agency that is rife with conflicts of interest? If the stem cell folks decide to go ahead and ask the people of California for more money for research, will the proposition they write be more at aimed at curing diseases (in which case research using the most promising approaches, whether stem cell-based or not, will be considered for funding) or will it be equally aimed at funding their own labs and thus promoting their own careers (including salaries)?
Friday, December 20, 2013
Tuesday, December 17, 2013
My car's gas door
I was pulling out of the gas station yesterday and this scruffy looking guy drives up behind me in his old beater and starts energetically gesticulating. I didn't know what to make of this and thought he was probably angry at me for some inadvertent slight. He got out of his car and walked rapidly towards mine. Oh Oh.
Then he reaches toward my car and . . . shuts my gas cap cover--once again I accidentally left it open (not the cap; the door)--gives me a thumbs-up and walks back to his car.
I don't know why--maybe because I'm getting older--I forget to close the gas door every now and then. Some kind person always alerts me or, more often, runs up to my car and closes it themselves. It's almost always someone driving an older or fairly downscale car. I have never once left a gas station with the door open. It's a small thing, but anything that provides a reason for optimism is good.
Then he reaches toward my car and . . . shuts my gas cap cover--once again I accidentally left it open (not the cap; the door)--gives me a thumbs-up and walks back to his car.
I don't know why--maybe because I'm getting older--I forget to close the gas door every now and then. Some kind person always alerts me or, more often, runs up to my car and closes it themselves. It's almost always someone driving an older or fairly downscale car. I have never once left a gas station with the door open. It's a small thing, but anything that provides a reason for optimism is good.
Thursday, December 12, 2013
Recipe for further decreasing the popularity of the Affordable Care Act/Obamacare
Here is a good way for opponents of Obamacare to decrease greatly its already low approval ratings:
1. Hold a panel discussion or debate on the Affordable Care Act and its implementation.
2. Ensure that Ezekiel Emanuel represents the pro-Obamacare side and, as a bonus, that people know that he is one of the Act's key architects.
3. Ensure that there is an audience that includes independent/undecided/agnostic and/or uninformed individuals.
4. Go to step 1.
footnote:
The first time I tuned in to hear this guy interviewed, I was looking forward to a dispassionate, balanced and nuanced discussion by a fellow physician. Wow, was I surprised, starting with the first sentence out of his mouth. He comes across as a political hack, and a very bad one at that: having no clue how to win over the audience or how to suppress his overbearing and obnoxious demeanor. Dr. Emanuel leaves no doubt that he thinks he is smarter than us and knows what is best for us. He seems to personify one of those "omnipotent moral busybodies" referenced in the prior post.
1. Hold a panel discussion or debate on the Affordable Care Act and its implementation.
2. Ensure that Ezekiel Emanuel represents the pro-Obamacare side and, as a bonus, that people know that he is one of the Act's key architects.
3. Ensure that there is an audience that includes independent/undecided/agnostic and/or uninformed individuals.
4. Go to step 1.
footnote:
The first time I tuned in to hear this guy interviewed, I was looking forward to a dispassionate, balanced and nuanced discussion by a fellow physician. Wow, was I surprised, starting with the first sentence out of his mouth. He comes across as a political hack, and a very bad one at that: having no clue how to win over the audience or how to suppress his overbearing and obnoxious demeanor. Dr. Emanuel leaves no doubt that he thinks he is smarter than us and knows what is best for us. He seems to personify one of those "omnipotent moral busybodies" referenced in the prior post.
Monday, November 25, 2013
A Prescient Thought by C.S. Lewis
The 50th anniversary of the death of C.S. Lewis was three days ago (the same day as the 50th anniversary of the death of JFK). I saw the passage from his writings that I have pasted below in a number of different articles and blog posts noting the occasion, including one by Steven Hayward (currently a scholar at the University of Colorado). As Hayward notes, it was prescient:
- Of all tyrannies, a tyranny sincerely exercised for the good of its victims may be the most oppressive. It would be better to live under robber barons than under omnipotent moral busybodies. The robber baron’s cruelty may sometimes sleep, his cupidity may at some point be satiated; but those who torment us for our own good will torment us without end for they do so with the approval of their own conscience.
"Hooey" Part 2: Harold Varmus Weighs In
How hard is it going to be to change the culture of scientists judging their peers by whether they make the effort to get their work in the journals Cell, Science etc.? I don't know. Based on the discussions of grants and investigators that took place at the most recent NIH study section (meeting of scientists to evaluate NIH grant applications) I attended, the tendancy of many towards judgments based on controversial measurements of journal prestige is well-ingrained. This bias was discussed in my last post.
I don't want to belabor the point, but I will anyway. This is from a recent article in Science on the prominent biomedical scientist Harold Varmus. He has held a number of prominent positions, and is now head of the National Cancer Institute:
Incidentally, I didn't realize until reading the article that Varmus was an important player in bringing about the doubling of the NIH budget over 5 years beginning about 1999. Paradoxically, this doubling contributed greatly to the subsequent funding woes, now worse than ever. Indeed, the article candidly states that the doubling helped bring about today's funding problems. Varmus claims that the doubling wasn't a mistake: he knew that the rapid increase in the NIH budget could cause problems but thought these could be avoided by facilitating a "soft landing." This "soft landing" was to be afforded by continuing budget increases that "kept pace with rising costs . . . ." This was plainly naive. How could anyone who observes how the government operates expect this type of long-term rational budgeting? Of course there was no soft landing. The biomedical work force and the number of new grants funded was greatly expanded, but these good times were, sure enough, followed my a massive hangover when it turned out there wasn't enough money to keep the party going.
I don't want to belabor the point, but I will anyway. This is from a recent article in Science on the prominent biomedical scientist Harold Varmus. He has held a number of prominent positions, and is now head of the National Cancer Institute:
- Varmus also wants to address what he calls the "flawed values system" that the competitive atmosphere has spawned. He laments that researchers feel they will win funding only if they publish in top journals such as Science, Nature, and Cell. At NCI, he is pilot-testing a way to change this part of the scientific culture: by revising the "biosketch," the summary of a researcher's record that accompanies a grant proposal. Varmus wants to replace a section that now lists major publications with a narrative describing the investigator's five major accomplishments.This approach, already used by the Howard Hughes Medical Institute (HHMI), should not only discourage reviewers from assessing their colleagues based only on where they're published; it will also help researchers on large teams whose names are buried in a list of authors receive the credit they deserve, Varmus says. And he thinks that easing the rush to publish in high-impact journals might help address a much-discussed problem: that many NIH-funded studies have proved difficult to reproduce. (emphasis mine)
Incidentally, I didn't realize until reading the article that Varmus was an important player in bringing about the doubling of the NIH budget over 5 years beginning about 1999. Paradoxically, this doubling contributed greatly to the subsequent funding woes, now worse than ever. Indeed, the article candidly states that the doubling helped bring about today's funding problems. Varmus claims that the doubling wasn't a mistake: he knew that the rapid increase in the NIH budget could cause problems but thought these could be avoided by facilitating a "soft landing." This "soft landing" was to be afforded by continuing budget increases that "kept pace with rising costs . . . ." This was plainly naive. How could anyone who observes how the government operates expect this type of long-term rational budgeting? Of course there was no soft landing. The biomedical work force and the number of new grants funded was greatly expanded, but these good times were, sure enough, followed my a massive hangover when it turned out there wasn't enough money to keep the party going.
Friday, November 15, 2013
A follow-up to the previous post regarding "hooey" in the scientific literature
I was talking to a prominent, accomplished biochemist at my institution about a possible collaboration. I mentioned a key paper supporting the scientific premise, and she asked me where it was published. When I gave her the name of the solid but non-prestige journal where it appeared, she said something along the lines of: "Oh good, it wasn't in Cell. That means its not a bunch of hooey." My paraphrasing is accurate, but the only word I distinctly remember is "hooey." Hence, the title of this follow-up to the immediately preceding post.
A surprisingly huge amount of BS ends up in the scientific literature. Many of the reasons for this are well-known and fairly obvious: for example, intense pressures to publish, difficulties publishing negative results, and academic and grant review committees that simply count numbers of papers published rather than assess content and contribution. Given the competition and politics involved in publishing in the very highest prestige journals (such as Cell), is it any wonder that misrepresentation and outright fraud is even more prevalent in these periodicals? Leaders in the field are urging us to stop paying attention to measurements of journal prestige and focus more on the content of what is published: basically, to stop the games surrounding publishing in Cell, Science, etc. This is highly commendable. But it is going to be hard to change this attribute of biomedical scientific culture.
In any case, yet more articles have come out accurately reporting on what is becoming less our dirty little secret and more our public scandal. Yet another article. And a video discussion.
Monday, July 29, 2013
Cheating, tweaking the data and the view of academic biomedical output from industry
I talk occasionally with an exceptionally bright former Ph.D. student of mine who works now in pharma. I wanted my next post to be positive--there is no lack of good things to say about the nation's biomedical research enterprise--but a conversation I just had with him prompted this post instead.
My conversation with my former student exactly mirrored discussions I have had with other scientists in pharma and biotech in this regard: a high proportion of the output from academic labs can't be reproduced and is thus worse than useless. "Worse" because it sends companies down dead-end avenues, wasting money and scientific talent that otherwise could be pursuing potential disease therapies with a chance of working. An article in the Wall Street Journal, quoting Bruce Alberts (a prominent scientist and former editor of a prestigious research journal), puts it this way:
My conversation with my former student exactly mirrored discussions I have had with other scientists in pharma and biotech in this regard: a high proportion of the output from academic labs can't be reproduced and is thus worse than useless. "Worse" because it sends companies down dead-end avenues, wasting money and scientific talent that otherwise could be pursuing potential disease therapies with a chance of working. An article in the Wall Street Journal, quoting Bruce Alberts (a prominent scientist and former editor of a prestigious research journal), puts it this way:
Two years ago, a group of Boston researchers published a study describing how they had destroyed cancer tumors by targeting a protein called STK33. Scientists at biotechnology firm Amgen Inc. quickly pounced on the idea and assigned two dozen researchers to try to repeat the experiment with a goal of turning the findings into a drug.
It proved to be a waste of time and money. After six months of intensive lab work, Amgen found it couldn't replicate the results and scrapped the project.
I was disappointed but not surprised," says Glenn Begley, vice president of research at Amgen of Thousand Oaks, Calif. "More often than not, we are unable to reproduce findings" published by researchers in journals.
This is one of medicine's dirty secrets: Most results, including those that appear in top-flight peer-reviewed journals, can't be reproduced. "It's a very serious and disturbing issue because it obviously misleads people" who implicitly trust findings published in a respected peer-reviewed journal, says Bruce Alberts, editor of Science. . . .
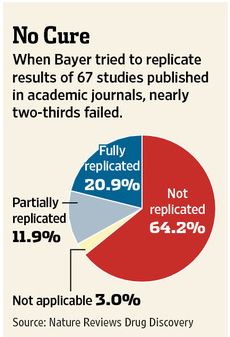
Drug manufacturers rely heavily on early-stage academic research and can waste millions of dollars on products if the original results are later shown to be unreliable. Patients may enroll in clinical trials based on conflicting data, and sometimes see no benefits or suffer harmful side effects.The WSJ article cites a study by the pharmaceutical company Bayer that found that company scientists had to halt 64% of early drug projects based claims in the literature due to inability to replicate published results:
A lot has been written about scientific fraud and how (unsurprisingly) it is probably more prevalent in the highest-prestige journals, about how the scientific literature is biased towards positive results and about the pressures of "publish or perish." I don't have anything new to say about these pressures on academic scientists: pressures that underlie the problem of there being so much garbage in the literature. I will only say this: the "soft money" system that makes scientists' livelihood dependent on winning grants plus the current brutal funding environment is a perfect formula for ensuring increased levels of scientific cheating and the resulting waste and damage to efforts to cure diseases.
Friday, July 19, 2013
Learning from Spitzer and Weiner
When I'm in the hospital being a doctor, I'm treated respectfully by staff, patients, students, nurses, other docs, etc. My job entails interacting with others in a professional manner and working with them towards common goals. There is a hierarchy on the hospital wards and in clinic, and I am generally at or near the top. Being constantly critiqued by colleagues is not part of clinical work.
On the other hand, when I'm wearing my academic researcher hat, I'm constantly being critiqued, evaluated, scored, criticised, etc. In theory, it's my academic and scholarly work that's being scrutinized, but it's hard not to take it personally. I am subject to scrutiny when I submit manuscripts for publication, when I'm considered for academic promotion and when I submit grant applications. Part of being a molecular biologist is being told your grant is not good enough to be funded, your manuscript needs more work or is outright rejected, and receiving other various sorts of criticism--usually anonymous--on a frequent basis. Grants, of course, do get funded, but rejection is a more common outcome. Manuscripts do get published, but again rejection is frequent. When papers are not rejected, there is often harsh criticism of the submitted draft: ok, not necessarily harsh, but to those without thick skin, even gentle criticism can often sound harsh. It helps greatly to have thick skin in this business*.
In my quest for ways to thicken my skin, I've found Anthony Weiner and Eliot Sptizer to be inspirational. If I had done what they had and had been subject to the same public humiliation and condemnation, I am not sure how I would ever have overcome the embarrassment. I can imagine hiding in a closet and wanting to disappear. If I were out in public, I would constantly be thinking about what other people were likely thinking about me. In short, it would be a disaster for my self-esteem. Weiner and Spitzer, however, are back to work in politics, out on the campaign trail and seemingly with their high regard for themselves intact, with nary a hint of shame. This is the pinnacle of thick skin, of unshakable self-esteem. And guess what: both have very strong chances of winning. Spitzer and Weiner should be an inspiration for every bioscientist who has ever moped for more than a couple of hours after a grant or manuscript rejection (which means, I think, a great many of us).
*DrugMonkey put it more succinctly:
On the other hand, when I'm wearing my academic researcher hat, I'm constantly being critiqued, evaluated, scored, criticised, etc. In theory, it's my academic and scholarly work that's being scrutinized, but it's hard not to take it personally. I am subject to scrutiny when I submit manuscripts for publication, when I'm considered for academic promotion and when I submit grant applications. Part of being a molecular biologist is being told your grant is not good enough to be funded, your manuscript needs more work or is outright rejected, and receiving other various sorts of criticism--usually anonymous--on a frequent basis. Grants, of course, do get funded, but rejection is a more common outcome. Manuscripts do get published, but again rejection is frequent. When papers are not rejected, there is often harsh criticism of the submitted draft: ok, not necessarily harsh, but to those without thick skin, even gentle criticism can often sound harsh. It helps greatly to have thick skin in this business*.
In my quest for ways to thicken my skin, I've found Anthony Weiner and Eliot Sptizer to be inspirational. If I had done what they had and had been subject to the same public humiliation and condemnation, I am not sure how I would ever have overcome the embarrassment. I can imagine hiding in a closet and wanting to disappear. If I were out in public, I would constantly be thinking about what other people were likely thinking about me. In short, it would be a disaster for my self-esteem. Weiner and Spitzer, however, are back to work in politics, out on the campaign trail and seemingly with their high regard for themselves intact, with nary a hint of shame. This is the pinnacle of thick skin, of unshakable self-esteem. And guess what: both have very strong chances of winning. Spitzer and Weiner should be an inspiration for every bioscientist who has ever moped for more than a couple of hours after a grant or manuscript rejection (which means, I think, a great many of us).
*DrugMonkey put it more succinctly:
I think our career / academics sets an environment in which you are constantly told you aren't doing quite enough, aren't quite excellent/brilliant enough and gee, we could probably get along without you, chumpie.
Saturday, July 13, 2013
Some doubts arising about the Medical Scientist Training Program? Part 2
An NIH Physician-Scientist Workforce Working Group has been formed and charged with gathering data and making recommendations about how to best sustain the physician-scientist biomedical workforce. The Physician-Scientist Working Group has not met yet, but there was a discussion regarding its goals at the June meeting of the Advisory Committee to the NIH Director (ACD). You can view a video of the ACD meeting here; you may want to skip right to the part about the Physician-Scientist Workforce Working Group. Most of the preceding discussion focuses on gloomy budgetary news and the resulting career difficulties facing biomedical researchers. The relevant segment begins at about the hour thirty-one minute (1:31) mark and runs about 10 minutes.
In Part 1 of this post, I noted that questions about the future of the MSTP program are being raised at the highest levels of the NIH. By "highest levels" I meant by the NIH Director himself. The Director, Francis Collins, asked the first question about the working group, which was whether there would be a focus on the "whole question about MD/Ph.D. training programs as a major part of [the working group's] deliberations." This is because "there are folks who are really beginning to wonder if we did the right thing by making this [MD/PhD training programs] such a centerpiece of our effort to train physician-researchers." Interesting.
The Advisory Committee and Dr. Collins should be lauded for instigating this analysis of physician-scientist training. As I alluded to in Part 1, I think the data may show that a surprisingly large fraction of MD/Ph.D. graduates end up in positions in which the benefit derived from the Ph.D. training, if any, is far outweighed by the cost in time and in taxpayer funds of that training. Indeed, the representative of the working group noted that combined clinical degree/PhD programs training dentist-researchers and veterinarian-researchers seem to be more successful than MD/PhD programs in turning out biomedical clinician-researchers. In any case, it will be interesting to see the data when it becomes available.
In Part 1 of this post, I noted that questions about the future of the MSTP program are being raised at the highest levels of the NIH. By "highest levels" I meant by the NIH Director himself. The Director, Francis Collins, asked the first question about the working group, which was whether there would be a focus on the "whole question about MD/Ph.D. training programs as a major part of [the working group's] deliberations." This is because "there are folks who are really beginning to wonder if we did the right thing by making this [MD/PhD training programs] such a centerpiece of our effort to train physician-researchers." Interesting.
The Advisory Committee and Dr. Collins should be lauded for instigating this analysis of physician-scientist training. As I alluded to in Part 1, I think the data may show that a surprisingly large fraction of MD/Ph.D. graduates end up in positions in which the benefit derived from the Ph.D. training, if any, is far outweighed by the cost in time and in taxpayer funds of that training. Indeed, the representative of the working group noted that combined clinical degree/PhD programs training dentist-researchers and veterinarian-researchers seem to be more successful than MD/PhD programs in turning out biomedical clinician-researchers. In any case, it will be interesting to see the data when it becomes available.
Tuesday, July 9, 2013
Maybe some doubts arising about the Medical Scientist Training Program? Part 1
I recently completed a several-year stint on my institution's Medical Scientist Training Program (MSTP) admissions committee. The MSTP is an NIH-funded program that pays for combined M.D./Ph.D. training at various research-oriented medical schools. The applications I saw--from the subset of candidates who were offered interviews--were highly (scarily) impressive: they sometimes (OK, often) made me wonder whether I would have been admitted had I applied in recent years.
The applicants I interviewed uniformly stated they envisioned a career in academic medicine with something like 20% of time devoted to clinical work and the rest being devoted to research (with teaching and administrative work also thrown into the mix). This distribution of effort conforms to the classic model of an academic physician-scientist. Out of curiosity (not as part of the formal interview), I asked a few of the applicants if they knew where their salary would typically come from if they pursued such a career. I was surprised that only one applicant (of the four I asked) was familiar with "soft money" (this applicant's parent was an academic physician).
I stumbled upon an online student forum with many participants applying to MSTP programs or at various stages of MD/Ph.D. training. It's not surprising to see that after they learn about the soft money system and become aware of its downsides, many of the trainees begin to reevaluate things, thinking much more concretely about how they want to structure their careers and about trade-offs involving risk, stress, job security, etc. We should probably ensure that students contemplating applying for MSTP positions are made aware of the practical realities of a career as a clinician-scientist up front.
My impression--based not on any formal analysis but rather on my first-hand knowledge of the career paths of other MD/Ph.D grads and my perusal of residency match and alumni information on the MSTP websites of various medical schools--is that a large fraction of MD/Ph.D. graduates go on to careers in which the ~4 years of intensive research training that goes into the Ph.D. is unnecessary and a waste of public funds. This could be the subject of an entire post or two, and I'm not going to go into detail here; just one observation along these lines. The nature of my graduate school work would have made me an ideal candidate for a dermatology residency. My research mentor (himself a physician-scientist) made it clear to me that he hoped I did not take this route. Why? Because, I would encounter sirens, the lifestyle and pay of dermatology private practice, that would lure my research career to its doom. As others have noted, it seems now that an increasing number of MD/Ph.D. candidates leverage the caché of their Ph.D. degrees to gain admittance to competitive residency programs in clinical specialties--such as dermatology, ophthalmology and radiology-- known for good lifestyle and lucrative salaries. Over 40% of MD/PhD graduates choosing dermatology, ophthalmology or radiology, for example, end up in private practice.
I recently learned that there are people paying attention attention to all this and that questions about the future of the MSTP program are being raised at the highest levels of the NIH. I will provide specifics in my next post.*
*Update: part 2 now posted.
The applicants I interviewed uniformly stated they envisioned a career in academic medicine with something like 20% of time devoted to clinical work and the rest being devoted to research (with teaching and administrative work also thrown into the mix). This distribution of effort conforms to the classic model of an academic physician-scientist. Out of curiosity (not as part of the formal interview), I asked a few of the applicants if they knew where their salary would typically come from if they pursued such a career. I was surprised that only one applicant (of the four I asked) was familiar with "soft money" (this applicant's parent was an academic physician).
I stumbled upon an online student forum with many participants applying to MSTP programs or at various stages of MD/Ph.D. training. It's not surprising to see that after they learn about the soft money system and become aware of its downsides, many of the trainees begin to reevaluate things, thinking much more concretely about how they want to structure their careers and about trade-offs involving risk, stress, job security, etc. We should probably ensure that students contemplating applying for MSTP positions are made aware of the practical realities of a career as a clinician-scientist up front.
My impression--based not on any formal analysis but rather on my first-hand knowledge of the career paths of other MD/Ph.D grads and my perusal of residency match and alumni information on the MSTP websites of various medical schools--is that a large fraction of MD/Ph.D. graduates go on to careers in which the ~4 years of intensive research training that goes into the Ph.D. is unnecessary and a waste of public funds. This could be the subject of an entire post or two, and I'm not going to go into detail here; just one observation along these lines. The nature of my graduate school work would have made me an ideal candidate for a dermatology residency. My research mentor (himself a physician-scientist) made it clear to me that he hoped I did not take this route. Why? Because, I would encounter sirens, the lifestyle and pay of dermatology private practice, that would lure my research career to its doom. As others have noted, it seems now that an increasing number of MD/Ph.D. candidates leverage the caché of their Ph.D. degrees to gain admittance to competitive residency programs in clinical specialties--such as dermatology, ophthalmology and radiology-- known for good lifestyle and lucrative salaries. Over 40% of MD/PhD graduates choosing dermatology, ophthalmology or radiology, for example, end up in private practice.
I recently learned that there are people paying attention attention to all this and that questions about the future of the MSTP program are being raised at the highest levels of the NIH. I will provide specifics in my next post.*
*Update: part 2 now posted.
Thursday, June 27, 2013
Ignoring the demoninator
Grant Reviewer A: "In the past 4 years investigator X has been moderately productive, having published 5 research papers."
Grant Reviewer B: "Applicant Z has been highly productive, having published 16 papers over the past 4 years."
Which investigator would likely make better use of additional funds? Who should get the better score? Answer: it makes no sense to try to answer these questions with this data alone (we'll ignore the issue of whether number of papers is a valid measurement of output: it's how the game is all-too often played). I'd be embarrassed if someone from the business world--where there is intense focus on the efficient deployment of capital--were to sit in on one of the study sections I've attended and critically analyze how bioscientists evaluate productivity. In general, we comment on the numerator and pay scant attention to the denominator. Would a manager allocate additional funds for production at a plant that turns out 10,000 light bulbs per day at a cost of $10,000 or a plant that turns out 2,000 at a cost of $600? Would the the decision be made after looking at the numerators (10,000 and 2,000) alone?
In my experience (service on several different NIH study sections and good knowledge of how reviews for academic promotion proceed at several different institutions), little or no attention is ever given to the denominator: to output per dollar. Is someone who publishes 15 papers using $4,000,000 of public funds and, say, 10 postdocs and grad students (the numbers given here are just for illustration and easy comparison) more meritorious than an investigator who publishes 5 papers using $750,000 and 2 postdocs/grad students? Who is making more efficient use of public or charitable funds? Who is getting the trainees in their labs more first author papers? (Remember, we're ignoring the issue of whether number of papers is a fair measurement of productivity.)
Renewal applications list all the papers attributable to the grant proposed for renewal, but this listing, in its current incarnation, is of little use. There is no way of knowing how much money from any particular grant was spent on the science in any particular paper. Investigators attribute individual papers to multiple grants. An investigator might make a small contribution to a collaborator's project and associate the resulting paper with one or all of her grants. Money and lab supplies are fungible. Supplies, personnel and equipment in any one lab get intermixed: there is not a wall separating each project. Unless more detailed accounting is required--and there wouldn't be very many investigators happy about the huge increase in record keeping that would be required--perhaps the best way of measuring how efficiently a lab uses funds is to look carefully at total money in versus total research out. Attention should also be paid to the fact that there seems to be an inflection point (~$750,000 per annum in total funding) beyond which total productivity per dollar begins to decline (the link leads to a good example of an analysis of productivity where attention is paid to funds expended).
Molecular biologists engage in highly complex data analysis in their laboratories. It is interesting that when when we travel to grant review sessions or sit on academic committees, we evaluate productivity in such a haphazard and inconsistent manner. Grant dollars are in short supply these days. It would make sense to evaluate how efficiently they are used in a more sophisticated, business-like manner.
(The need to distribute funds wisely also applies to grants to New Investigators: see prior post).
Grant Reviewer B: "Applicant Z has been highly productive, having published 16 papers over the past 4 years."
Which investigator would likely make better use of additional funds? Who should get the better score? Answer: it makes no sense to try to answer these questions with this data alone (we'll ignore the issue of whether number of papers is a valid measurement of output: it's how the game is all-too often played). I'd be embarrassed if someone from the business world--where there is intense focus on the efficient deployment of capital--were to sit in on one of the study sections I've attended and critically analyze how bioscientists evaluate productivity. In general, we comment on the numerator and pay scant attention to the denominator. Would a manager allocate additional funds for production at a plant that turns out 10,000 light bulbs per day at a cost of $10,000 or a plant that turns out 2,000 at a cost of $600? Would the the decision be made after looking at the numerators (10,000 and 2,000) alone?
In my experience (service on several different NIH study sections and good knowledge of how reviews for academic promotion proceed at several different institutions), little or no attention is ever given to the denominator: to output per dollar. Is someone who publishes 15 papers using $4,000,000 of public funds and, say, 10 postdocs and grad students (the numbers given here are just for illustration and easy comparison) more meritorious than an investigator who publishes 5 papers using $750,000 and 2 postdocs/grad students? Who is making more efficient use of public or charitable funds? Who is getting the trainees in their labs more first author papers? (Remember, we're ignoring the issue of whether number of papers is a fair measurement of productivity.)
Renewal applications list all the papers attributable to the grant proposed for renewal, but this listing, in its current incarnation, is of little use. There is no way of knowing how much money from any particular grant was spent on the science in any particular paper. Investigators attribute individual papers to multiple grants. An investigator might make a small contribution to a collaborator's project and associate the resulting paper with one or all of her grants. Money and lab supplies are fungible. Supplies, personnel and equipment in any one lab get intermixed: there is not a wall separating each project. Unless more detailed accounting is required--and there wouldn't be very many investigators happy about the huge increase in record keeping that would be required--perhaps the best way of measuring how efficiently a lab uses funds is to look carefully at total money in versus total research out. Attention should also be paid to the fact that there seems to be an inflection point (~$750,000 per annum in total funding) beyond which total productivity per dollar begins to decline (the link leads to a good example of an analysis of productivity where attention is paid to funds expended).
Molecular biologists engage in highly complex data analysis in their laboratories. It is interesting that when when we travel to grant review sessions or sit on academic committees, we evaluate productivity in such a haphazard and inconsistent manner. Grant dollars are in short supply these days. It would make sense to evaluate how efficiently they are used in a more sophisticated, business-like manner.
(The need to distribute funds wisely also applies to grants to New Investigators: see prior post).
Friday, June 21, 2013
Sick as stink
Do medical residents still use the term "sick as stink?" It was how we sometimes conveyed that a patient was in very bad shape back when I was a resident.
A vivid memory of my medical school years is AIDS patients who indeed were sick as stink, very much so. They were most often--at least in my memory--young, gay adult men who, before becoming infected with HIV, were fit and healthy (in contrast to the IV drug abusers, the other major HIV patient population). The AIDS patients presented with a variety of otherwise unusual ailments, often infectious, mostly terrible. My memory is of people who were generally in the prime of their lives and then became horribly ill. One of my first experiences on the wards was seeing a newly-admitted patient walking up to the wards, still in street clothes, with his obviously caring partner--a really nice couple--and thinking that he didn't look that sick and would likely be going home in a few days. He died of pneumocysitis pneumonia a few days later.
Do residents still commonly see Kaposi's sarcoma. pneumocystis pneumonia, toxoplasmosis, cryptococcal meningitis and the rest of the terrible encyclopedia of diseases of immune deficiency that accompany AIDS? It has been amazing to witness the progress against HIV, with patients now having life expectancies approaching normal. Do lawyers witness similar amazing, life-giving advances over the years in their profession? Business consultants?
This is an important part of the big picture of being a physician-scientist: this career makes you an essential part of an enterprise that can really accomplish great things. Advances made in biomedical research reduce human suffering and contribute in a big and permanent way to human progress. This is not a bad thing to think about on those days when I am left wondering "how did I get myself into this? Why didn't I become an attorney/investment banker/Beverly Hills dermatologist like my college classmates?"
A vivid memory of my medical school years is AIDS patients who indeed were sick as stink, very much so. They were most often--at least in my memory--young, gay adult men who, before becoming infected with HIV, were fit and healthy (in contrast to the IV drug abusers, the other major HIV patient population). The AIDS patients presented with a variety of otherwise unusual ailments, often infectious, mostly terrible. My memory is of people who were generally in the prime of their lives and then became horribly ill. One of my first experiences on the wards was seeing a newly-admitted patient walking up to the wards, still in street clothes, with his obviously caring partner--a really nice couple--and thinking that he didn't look that sick and would likely be going home in a few days. He died of pneumocysitis pneumonia a few days later.
Do residents still commonly see Kaposi's sarcoma. pneumocystis pneumonia, toxoplasmosis, cryptococcal meningitis and the rest of the terrible encyclopedia of diseases of immune deficiency that accompany AIDS? It has been amazing to witness the progress against HIV, with patients now having life expectancies approaching normal. Do lawyers witness similar amazing, life-giving advances over the years in their profession? Business consultants?
This is an important part of the big picture of being a physician-scientist: this career makes you an essential part of an enterprise that can really accomplish great things. Advances made in biomedical research reduce human suffering and contribute in a big and permanent way to human progress. This is not a bad thing to think about on those days when I am left wondering "how did I get myself into this? Why didn't I become an attorney/investment banker/Beverly Hills dermatologist like my college classmates?"
A Perspective with a misleading title
The New England Journal of Medicine prints its table of contents on the front cover. When my wife pulled the most recent issue from our mailbox and saw the article title "The Role of the NIH in Nurturing Clinician-Scientists," she naturally thought I would be interested. I was.
The Perspective article begins by stating the value of physician scientists. I have no quibble with this. Then it makes the oft-repeated point that increasingly, physicians don't want to do this basic research thing anymore. I wonder why?
Then the really disheartening part: the remaining 90% of the article turns out to mostly a pitch for a new NIH program supporting a total of 20 new physician investigators at any one time. Let's think about this: 20 investigators at a time divided by the 10 to 12 years that the program spans (yes: the lucky few will get 10 to 12 years of support, including a 5 to 7 year stint on the NIH campus). So,1 to 2 new physician-investigators per year will enter the workforce via this pipeline. And this merits 2 pages of valuable real estate at the front of the NEJM?
The title of the article led me to believe that there might be a more general discussion of how the NIH could "nurture" physician-scientists at all stages of their careers. This seems to be especially topical in these tight times. There was no such discussion.
How many highly-trained (at great cost, mostly borne by taxpayers) physician-scientists at various stages of their careers or newly-trained MD-PhDs will leave basic or translational science each year that 1 or 2 new trainees are accepted into this new NIH program? Would it be more cost effective, instead of bringing new investigators into the system, to, say, encourage newly trained MD-PhDs to stay in research (rather than going into, for example, lucrative clinical practices, as many do)? The investment in already-trained physician-scientist should be protected by addressing some of the problems that are driving them away rather than initiating yet another training program.
The Perspective article begins by stating the value of physician scientists. I have no quibble with this. Then it makes the oft-repeated point that increasingly, physicians don't want to do this basic research thing anymore. I wonder why?
Then the really disheartening part: the remaining 90% of the article turns out to mostly a pitch for a new NIH program supporting a total of 20 new physician investigators at any one time. Let's think about this: 20 investigators at a time divided by the 10 to 12 years that the program spans (yes: the lucky few will get 10 to 12 years of support, including a 5 to 7 year stint on the NIH campus). So,1 to 2 new physician-investigators per year will enter the workforce via this pipeline. And this merits 2 pages of valuable real estate at the front of the NEJM?
The title of the article led me to believe that there might be a more general discussion of how the NIH could "nurture" physician-scientists at all stages of their careers. This seems to be especially topical in these tight times. There was no such discussion.
How many highly-trained (at great cost, mostly borne by taxpayers) physician-scientists at various stages of their careers or newly-trained MD-PhDs will leave basic or translational science each year that 1 or 2 new trainees are accepted into this new NIH program? Would it be more cost effective, instead of bringing new investigators into the system, to, say, encourage newly trained MD-PhDs to stay in research (rather than going into, for example, lucrative clinical practices, as many do)? The investment in already-trained physician-scientist should be protected by addressing some of the problems that are driving them away rather than initiating yet another training program.
Friday, June 7, 2013
Kinda scary
Up until very recently the very low rate of success of grant applications submitted to the NIH has been disturbing yet, to me, abstract. However, over the past week I have spoken to two different investigators whose grants were scored at around the 18th percentile (in other words, better than over 80% of the competing applications) and yet did not get funded. And one was a New Investigator. I had heard that only the top 8-14% or so of applications were winning funding, but these first-hand concrete examples really drove the ugly reality home. Remember that due to the soft money system investigators rely on grants to put food on the table (i.e., have an income). Hmmm . . . maybe it's time to dust off my stethoscope.
Thursday, May 30, 2013
A nasty little mystery of the mind
I just read an editorial in Science authored by the NIH Director and a couple of other NIH bigwigs plugging the new NIH BRAIN (yes, all caps) Initiative. The plan is to develop new technologies to figure out how our brains work. I have no opinion about the project in general, but there is one question I would very much like to see answered: why, as I grow older and my mind becomes less agile and my memory not as reliable, am I nevertheless able to recall every awkward or embarrassing moment, every uncomfortable instance, in my life as vividly as ever? It's as if the synaptic connections comprising these memories are super-glued together. The rest of my mind is held together by Elmer's.
Sunday, May 26, 2013
Cashing in on being an NIH "New Investigator"
Investigators fresh out of training have a hard time competing for grants against established scientists with proven track records and often backed by large, resource-rich laboratories and armies of postdoctoral fellows and grad students. This problem is compounded by the fact that the NIH grant review system has no formal metric--no system at all really--for just how efficiently these more senior investigators are using their research funds, a topic I won't delve into right now.
The NIH has made an effort to level the playing field for these newbies, who self-identify by checking a box on NIH grant applications indicating that they are a "New Investigator." This provides various significant benefits in the competitive grant review process. This is all for the best (although I guess one could argue that perhaps, given the current funding situation , the flow of investigators into NIH-grant funded research should be slowed).
So, we have these new investigators who have a minimal track record, and they are given a shot to prove themselves. But here's the thing: until they receive notification that one of their applications has been funded, they can submit as many grant applications as they want with the "New Investigator" box checked off . Furthermore, these young applicants can apply for special, very large, research awards only available to New Investigators.
Illustrative of the kinds of inefficiencies that result when an enormous government bureaucracy doles out public funds, there is no coordination within the NIH in regards to how multiple applications from the same New Investigator are handled. One part of the NIH can decide to take a chance and give the New Investigator a chance to prove him or herself by awarding them a grant without knowing the applicant has already been awarded funding by a different part. Brand new independent investigators with no track record of running their own research program or administering their own laboratory can suddenly find themselves showered with huge sums of NIH research funds.
As a result of this lack of coordination within the NIH, there are newly independent investigators who are simultaneously awarded two R01 grants along with a DP2 grant, which are very large grants targeted specifically to new investigators. Getting what is called in NIH parlance an "R01" grant is a big deal. Established scientists are finding it very difficult to get R01 grants funded these days.
Here is a real-life example of the grants awarded to one such new investigator all within a few months of each other (since they were all submitted prior to any of them being awarded, they were all accorded New Investigator status):
1. An R01 grant that will cost the NIH $329,000 per year over 5 years.
2. Another R01 grant that will cost the NIH $388,000 per year over 5 years
3. A special grant just for newbies, called a DP2: cost to NIH is $2,320,000 to be spent over 5 years.
So, this new investigator goes all at once from zero NIH funding to $5,905,000 to be spent over 5 years (note: about one third of this total goes directly to the investigator's university to cover overhead costs). And this in a time when established laboratories are closing due to an inability to get their R01 grants renewed. What do you think about that?
The NIH has made an effort to level the playing field for these newbies, who self-identify by checking a box on NIH grant applications indicating that they are a "New Investigator." This provides various significant benefits in the competitive grant review process. This is all for the best (although I guess one could argue that perhaps, given the current funding situation , the flow of investigators into NIH-grant funded research should be slowed).
So, we have these new investigators who have a minimal track record, and they are given a shot to prove themselves. But here's the thing: until they receive notification that one of their applications has been funded, they can submit as many grant applications as they want with the "New Investigator" box checked off . Furthermore, these young applicants can apply for special, very large, research awards only available to New Investigators.
Illustrative of the kinds of inefficiencies that result when an enormous government bureaucracy doles out public funds, there is no coordination within the NIH in regards to how multiple applications from the same New Investigator are handled. One part of the NIH can decide to take a chance and give the New Investigator a chance to prove him or herself by awarding them a grant without knowing the applicant has already been awarded funding by a different part. Brand new independent investigators with no track record of running their own research program or administering their own laboratory can suddenly find themselves showered with huge sums of NIH research funds.
As a result of this lack of coordination within the NIH, there are newly independent investigators who are simultaneously awarded two R01 grants along with a DP2 grant, which are very large grants targeted specifically to new investigators. Getting what is called in NIH parlance an "R01" grant is a big deal. Established scientists are finding it very difficult to get R01 grants funded these days.
Here is a real-life example of the grants awarded to one such new investigator all within a few months of each other (since they were all submitted prior to any of them being awarded, they were all accorded New Investigator status):
1. An R01 grant that will cost the NIH $329,000 per year over 5 years.
2. Another R01 grant that will cost the NIH $388,000 per year over 5 years
3. A special grant just for newbies, called a DP2: cost to NIH is $2,320,000 to be spent over 5 years.
So, this new investigator goes all at once from zero NIH funding to $5,905,000 to be spent over 5 years (note: about one third of this total goes directly to the investigator's university to cover overhead costs). And this in a time when established laboratories are closing due to an inability to get their R01 grants renewed. What do you think about that?
Sunday, May 19, 2013
Some great things about this job, Part 1
My job has a number of abstract benefits, such as the opportunity to work at the frontier of medical science and to carry out research that may eventually help those suffering from disease. These benefits are easy to ignore; they tend to get lost in the shuffle on a day-to-day basis. More concretely, looking at new, interpretable data, no matter how mundane, is always fun. Analyzing interesting results is even more fun. On a more practical note, I have great freedom to set my own schedule and hours. This is a particularly nice benefit since I have kids; I am usually able to easily adjust my schedule, for example, to stay home with them if they're ill or spend time with them if they have an odd day off. Molecular biology can be extraordinarily frustrating and there can be long periods of time where little progress is made. In rough stretches like this, I especially appreciate also being a physician. With patient care, I always feel like I've accomplished something; same goes for teaching.
Thursday, May 16, 2013
How can universities grant you tenure if they don't pay you?
Medical schools need full-time doctors to work in their hospitals and clinics; they also employ physicians who, because they carry out clinic-based research, can earn their salary by treating patients. You can recognize these docs by the word "clinical" in their titles, as in "clinical professor" or "professor of clinical (pick a medical specialty)." For whatever reason, these professors are subject to a system of evaluation and promotion that awkwardly overlaps that of a professor of, say, art history, but that's a topic for a later time.
This post is not about these clinically-oriented physicians, but rather about "tenure-track" physician faculty members who spend most of their time doing non-clinical/basic research.
This post is not about these clinically-oriented physicians, but rather about "tenure-track" physician faculty members who spend most of their time doing non-clinical/basic research.
"Tenure-track" physician-scientists are evaluated and promoted in exactly the same way as any other aspiring professor, for example the professor of art history I mentioned above. This means a period of time at the assistant professor level and then, after six or seven years max, it's either up or out. "Up" means tenure. Universities have basically handed over decision-making regarding tenure to their faculties. Which is to say, faculty committees set up to play an advisory role have become the de facto arbiters of tenure decisions, only rarely (at the universities I am most familiar with, in any case) being overruled by university chancellors or vice-chancellors. The fun part is that the final faculty committee to weigh-in is often a university-wide committee, comprised of professors of you-name-it (history, sculpture, engineering, music, physics and so on). If you think that it may not always be optimal to have, say, a professor of political science weighing in on the scientific output of a molecular biologist or, say, a Ph.D. molecular biologist commenting on the clinical service and teaching of an MD of MD-PhD, I would have to agree.
Though faculty members are subject to this promotion system throughout their career, the biggest step is the tenure decision. This is also a big step for the university, since, by giving someone tenure, they are committing to career-long employment of that individual. So, the assistant professor has to run this gauntlet, but, if successful, will thereafter have career-long economic security. Unless he or she is on a medical school faculty, in which case she will get all of the same stress and little or none of the resulting security (see my earlier post on soft money). I found this galling before I received tenure and, now that I have tenure, still think it is highly unfair. I was interested to learn that the major trade organization for professors, the American Association of University Professors (AAUP), has been clued in to this problem and is most displeased. They are insistent that "economic security" is an essential component of tenure. Here is some of what the AAUP has had to say on the matter (from the AAUP report "Tenure in the Medical School"):
- . . . . The 1940 Statement of Principles stipulates that tenure is a means not only to academic freedom, but also to “a sufficient degree of economic security to make the profession attractive to men and women of ability.” Except, as is sometimes the case, where the reward of rank and tenure is purely honorific, all tenured and tenure-track faculty should be guaranteed an assured minimum salary adequate to the maintenance of support at a level appropriate to faculty members in the basic sciences, and not merely a token stipend, . . .
(emphasis added)
and
- We question whether any institution of higher education or one of its components, whether the purpose be undergraduate, graduate, or professional education, can provide such educational quality without that reasonable assurance of stability that helps ensure the commitment of its faculty members to freedom of inquiry in teaching and research and to the preparation of its students.
(emphasis added)
Sunday, May 12, 2013
Soft money: how to hire a physician-scientist for free
You may think of university professors as having cushy jobs which--thanks to tenure--guarantee us a job and a salary (as you will see, this is not redundant) right up until retirement. This may be true for, say, professors of political science or English literature, but this is most definitely not the case for your typical academic biomedical scientist. In fact, not only do biomedical faculty not receive a guaranteed salary, they often receive no salary at all. You see, back when grant dollars were easier to come by, academic medical centers figured out that they could hire scientists and pay them only a small percentage of their salary, very often 0%. The professors' salaries would be mainly foisted off onto the granting agencies (mostly the National Institutes of Health). This was brilliant: universities could hire faculty virtually on a volunteer basis, agree to pay them X per year, pay them a fraction of X per year or zilch, and tell them they were on their own to scrounge up the rest. If the faculty member was lucky and had part of her salary paid by the hiring institution, they were said to receive "hard money." The rest is "soft money."
*link will download an Excel file from the NIH website
**see first comment for caveat regarding using a Google web search for quantitation in this manner
*** "my current favorite" except for the occasional political commentary, which is often uninformed and/or venomous.
This soft-money based system evolved at at time when over 30-40%* of NIH grant applications--and some years over 50%--were approved for funding. What happens when grant approval rates are closer to 10-15%? Here is one indicator: a Google search for "soft money" (not the political kind) and "stress" results in over 59,000 hits**. Considering also the vagaries of the grant review system, the soft-money system verges on cruelty. Highly-educated, generally very intelligent researchers are forced to compete against each other to be one of the few investigators selected for funding. Loss of research funding could very well equal loss of salary support and derailment of ones career. And people are wondering why physicians don't want to have biomedical research careers anymore?
As a physician-scientist, I am fortunate in that having to leave academia would result in an increase in my income, and it would not be hard to find a job as a clinician. If I'm stressed, I wonder how straight Ph.D. faculty members must feel? The 59,000 Google hits I mentioned above give some indication of this**. There is also much discussion of the current dire funding situation--the angst is almost palpable--and it's impact on medical school faculty careers at the blogs of other biomedical researchers, including my current favorite***.
*link will download an Excel file from the NIH website
**see first comment for caveat regarding using a Google web search for quantitation in this manner
*** "my current favorite" except for the occasional political commentary, which is often uninformed and/or venomous.
Thursday, May 9, 2013
Intro and Anonymity
Hello. This, my first foray into blogging, will include (in part) a behind-the-scenes glimpse of academic biomedical research that--I hope--will be of interest to you, dear reader, the taxpayer who pays for (almost) all this work. It may also be of interest to students pondering whether to spend most of their 20s in MSTP*/MD-PhD training and then, most likely, some of their early 30s in the requisite postdoctoral training. I also have a dirty little secret that I will divulge sometime in the future. Nothing illegal or unethical or related (directly) to science, but something that I don't talk about in polite academic company.
My decision to use a pseudonym was arrived at after a bit of deliberation. An important aspect of being an academic biomedical scientist is that your colleagues, most often acting in an anonymous capacity, have an incredible amount of influence over your career. The fates of your grant applications, the manuscripts you have submitted for publication and your applications for promotion, are, in general in the hands of individuals who are in no way invested in your career and who basically have free rein to indulge their whims and be swayed by their moods. Though my fellow scientists are almost always at pains to fair, they are, alas, human, each and every one of them, and subject to the same failings and imperfections of thought as are we all. In short, I don't want to have to worry about ticking off someone who will later sit in judgement over one of my manuscripts or grant applications. So I'll remain anonymous.
*MSTP, Medical Scientist Training Program: an NIH-funded program created to train physician-scientists at research-oriented medical schools around the country. Graduates earn both M.D. and Ph.D. degrees.
My decision to use a pseudonym was arrived at after a bit of deliberation. An important aspect of being an academic biomedical scientist is that your colleagues, most often acting in an anonymous capacity, have an incredible amount of influence over your career. The fates of your grant applications, the manuscripts you have submitted for publication and your applications for promotion, are, in general in the hands of individuals who are in no way invested in your career and who basically have free rein to indulge their whims and be swayed by their moods. Though my fellow scientists are almost always at pains to fair, they are, alas, human, each and every one of them, and subject to the same failings and imperfections of thought as are we all. In short, I don't want to have to worry about ticking off someone who will later sit in judgement over one of my manuscripts or grant applications. So I'll remain anonymous.
*MSTP, Medical Scientist Training Program: an NIH-funded program created to train physician-scientists at research-oriented medical schools around the country. Graduates earn both M.D. and Ph.D. degrees.
Subscribe to:
Comments (Atom)